Journal of Surgical Practice and Case Reports
Case Report Volume: 2 & Issue: 1
Case Report Volume: 2 & Issue: 1
The common neurological condition of Restless legs syndrome (RLS) is estimated to occur in some 4-15% of the population worldwide.2 Prevalence increases with age and is higher in females. Estimates of 10% Adults and 4% Children in the United States have presented with RLS symptoms. RLS has a distinct circadian rhythm with symptoms at presleep. RLS is linked to the periodic limb disorder that is characterized with flailing limbs. By contrast, RLS is characterized by leg movements in an up and down pattern with a sensory component of crawling sensations.5 There are considerable individual differences in the qualitative aspects of the leg movement but with RLS, all patients have the common experience of no identified trigger, inability to detour or stop the leg movements and discomfort ranging from sensory to cramping sensations. In summary, RLS is characterized as a sensorimotor disorder with unknown pathology with patient reports of an uncontrollable urge to move the legs in response to uncomfortable sensations.5
Questions about RLS symptoms are included on every sleep history interview. Also, RLS is underestimated in patient reports as the sensory/movement experience has familiar features of leg movements and is often not considered a pathology. Various stages of pregnancy, anemia, undiagnosed metabolic disorders such as Diabetes mellitus type 2, and anxiety disorder are a few of the co-occurring conditions which RLS must be distinguished from in diagnosis.7
Pathonomic indicators such as single nucleotide polymorphisms (BTBD9, MEIS1) are involved in the development of RLS.2,7 Autopsy reports have found a brain decrease in iron related to A11 cells groups.2,7 These contemporary science findings about RLS etiology advance the thinking on the diagnosis.8 However, the gaps in replications and clear consensus of models of the pathophysiology are still in construction. Despite this, current assessment approaches often include laboratory testing of Iron, review of patient medical history and medications that may cause RLS.9 An overnight polysomnogram sleep study (PSG) that includes leg leads in the setup is used to confirm the diagnosis. The first reporting of RLS if it is detected by the patient is often in mid-adulthood.2 The protocol for assessment and treatment of RLS is available from the American Association of Sleep Medicine (https://aasm.org).
If RLS is known or once it is diagnosed, the degree of disruption from symptoms to the patient’s quality of life is revealed. Oftentimes, the patient presents with sleep disturbances of sleep onset/sleep maintenance Insomnia. A correspondence between responses on the Short Form Health Survey (SF-36) scores of poor mental and physical health and severe RLS symptoms.2 The circadian rhythm of RLS occurs as pre-sleep events. As a sleeper falls asleep, the core body temperature drops slightly.5 It is this pre-sleep timing that corresponds with core body temperature reductions that cascades other biochemical events. Plasma dopamine and metabolite levels change with decreasing core body temperature changes.2,8 Further, studies have identified dopamine receptors sensitivity increases with nighttime levels of tubero-infundibular-dopaminergic system activity. And correlations variations in serum iron, CSF dopamine levels and severity of symptoms have been found.2,8 Thus, pharmacological treatments have been dopamine agonists to address these empirically/clinical changes in dopamine levels corresponding to RLS severity. However, dopamine agonists are no longer the first line of RLS treatment and are to be prescribed under specific conditions. The non-ergot derived dopamine agents are Pramipexole, Ropinirole, Rotigotine. Recently, alpha 2 gamma agonists have been identified as useful treatment approaches for RLS. Gabapentin and Pregabalin are alpha 2 gamma agonist used to treat RLS. In some cases, Levodopa is considered for treatment of RLS. The standard presentation is provided by the diagnosing physician of the pharmacological name, mechanism of action, potential side effects and a plan of what to do should they occur. Further, prescribing physicians may choose combinations of pharmacologic agents to address the action for patient symptom relief. The reader is directed to more comprehensive presentation of pharmacology to Katzung Basic & Clinical Pharmacology and https://aasm.org.
A new approach, non-invasive peripheral nerve stimulation (NPNS) is being investigated.1 In this, a stimulator is placed on the peroneal nerve site on each leg to provide a competing stimulus for afferent pathways of the sensorimotor pathway to the brain. Preliminary studies point to a success rate of 66%.1 As the NPNS is currently in clinical trials, there is some difficulty providing this resource as a treatment.
Behavioral treatments for RLS include a modification of Cognitive Behavior Therapy to address the sleepiness that is secondary to the fragment/abbreviated sleep of the RLS patient, supportive psychotherapy to address stress and coping skills, cognitive therapy focusing on thought distortions related to sleep and problem solving/time management for identified alert times of the day.5,6 Also, behavior therapy focuses on reinforcing behaviors related to sleep and health of the patient. A thorough psychological evaluation precedes the assignment and onset of therapy. The evaluation is to include a psychiatric symptom assessment, level of coping, level of readiness for change and motivation for therapy. With standard, psychometrically sound instruments in these areas of assessment, an interview and evaluation can be completed within a clinical hour. The therapy approaches mentioned, except for supportive psychotherapy, are topic focused and short term, typically four to eight sessions. The patient is usually responsible for not only the completion of any questionnaire but also the monitoring of sleep using a sleep log. The psychological evaluation is concurrent with the Physician interview or follows with a referral. To be clear, the first line of treatment is Physician interview, laboratory test, PSG if needed and a prescribed pharmacological agent. The behavioral treatments can co-occur with the prescribed pharmacological agent. An emphasis during CBTi or as a therapeutic approach, Rational Emotive Therapy approaches that focus on cognitive distortions/beliefs the patient may have, in this case, worries that one may not sleep tonight instead of relaxing to sleep are used.3,5,6
A 68-year-old white female, retired elementary school teacher, widowed living in a single home dwelling presented to the Insomnia clinic with severe difficulty falling asleep and staying asleep sometimes for the last thirty-five years. She said that she “powered” through her workday and welcomed the early dismissal of her workdays to come home and sit in her recliner chair to rest. Patient stated that now with retirement, her attention to her poor sleep quality is amplified. She denied daytime sleepiness. She denied napping but did show she has some poor recall of the television show (she thinks she drifts to short sleep) that she typically views from 5-9:30pm. She reported a 9:30pm to 5:30am bedtime for her work life and now, in the past three years, 9:30pm to 6am with returning to bed sometimes until 8 or 8:30 am with no napping. She reported that family members said she has a mildly loud snore. The patient lives alone, she has one grown daughter that lives nearby and visits in person once or twice a week and has constant phone/text contact. She reported spending her day with crafts, some lunches with friends and family and household upkeep and watching her granddaughter after school until 5pm. The patient sometimes visited out of state family members and dinners with friends and ex-coworkers.
The physician interview found sleep disturbance of Insomnia Sleep Onset. Sleep Maintenance Insomnia, Parasomnia, Narcolepsy and Sleep apnea were ruled out by the all night polysomnogram. The patient was prescribed a beta agonist medication to address the diagnosis made of RLS.9
The psychological evaluation named mild anxiety surrounding her health, loneliness and some chronic family discord with siblings and one other family member that upsets her. The patient report and one week of sleep log corroborated the first reporting of bedtime and wake times. She presented during the interview the pre-sleep pattern of viewing television after dinner from 5pm to bedtime and feeling that she falls asleep for a few minutes, wakes then falls asleep again during this time. Then, she explained, she has bursts of energy and finds it difficult to sit so she walks around her condominium and even sometimes up and down stairs. She finds that she can sit for a while –usually less than five minutes then the discomfort in both legs propels her to walk around.
The patient has had recent physical exam and laboratory work with no remarkable findings. She reported being a healthy eater with three meals some four to five hours apart. She has changed her sleep environment to adhere to good sleep hygiene. She denied tobacco, alcohol and recreational substance use. She reported some arthritis in her hands that limits her craft/art making activities that is relieved by OTC Tylenol. The patient added at the end of the interview, that recently on her way home from grocery shopping and sometimes after a visit with a family member or babysitting that she has had some strange behavior. She elaborated to state that she stops at casinos and offtrack betting establishments to place at first, small bets but recently in the last four months larger bets of $500 or more. The patient related this point in tears as she explained that she is worried she is out of control, has lost a considerable amount of money and does know why she is doing this as she never gambled before this time.
The patient’s dopamine agonist medications, (Pramipexole, a dopamine agonist), while intended for short term use to address RLS symptoms, the mechanism of action enhancing the dopamine pathway seemed to be concurrently stimulating the learning/reinforcement center of the dopamine pathway propelling her into reinforcement seeking behaviors. That initial flash of excitement or break in her routine/boredom may have had the unintended consequence of overstimulating the dopamine pathway thus propelling her to urge and seek behaviors of that reinforcement.2 This explanation was provided; the physician was notified of the aberrant behavior and an alternative pharmacological agent was prescribed.7 The patient responded to behavior intervention of readjusting her pleasant event schedule of reinforcement and to the Cognitive Behavior Therapy Insomnia treatment (CBTi) to address her sleep disturbance, enhance her sleep quality with sleep schedules, behavioral training in Mindfulness to train her relaxation skills and psychoeducation and problem solving approaches to address any distortions or assumptions about sleep health. She looked forward to her mindfulness relaxation training from the CBTi treatment. In the six weeks of CBTi, the patient missed one session but was compliant with her sleep logging throughout. Topics of basic sleep mechanisms, sleep hygiene and behavioral activating events were taught. Some of the therapeutic discussions were focused on the neuroscience issue of her medication reaction to improve her self-esteem doubts that the behaviors were not authentic personality behavior. The comorbid insomnia was sufficiently addressed with the CBTi sessions.4-6 The surprising side effect of the original prescription for RLS was remitted at once with the discontinuation of that prescription. Equally important, the patient’s RLS symptoms were reduced with the alternative prescription. Additionally, the patient has completed insurance processing and registration for stimulator therapy for her RLS which she would like to try instead of medications. Her sleep logs indicated positive changes to her comorbid Insomnia,5 from the CBTi and are reflected in Figure 1.
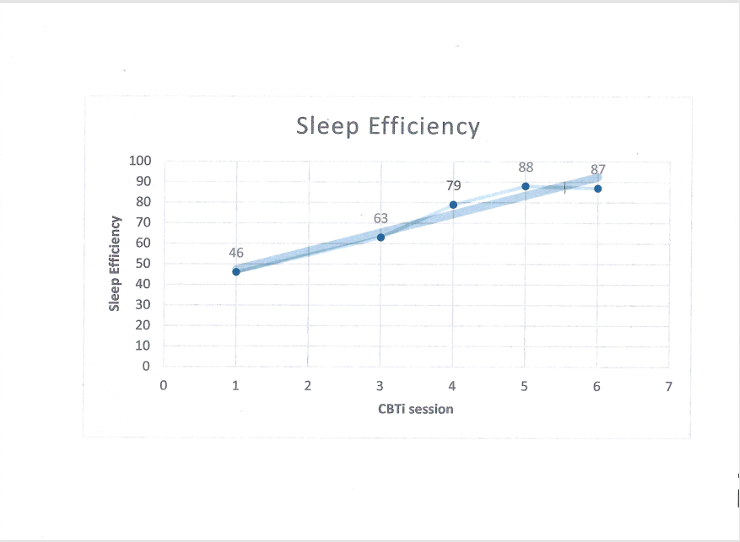
Figure 1. Sleep Efficiency over four weeks CBTi